Puskesmas, or community health centers, are relied on as the spearhead of community health service.
By
ATIKA WALUJANI MOEDJIONO
·3 minutes read
Kompas/Ferganata Indra Riatmoko
.
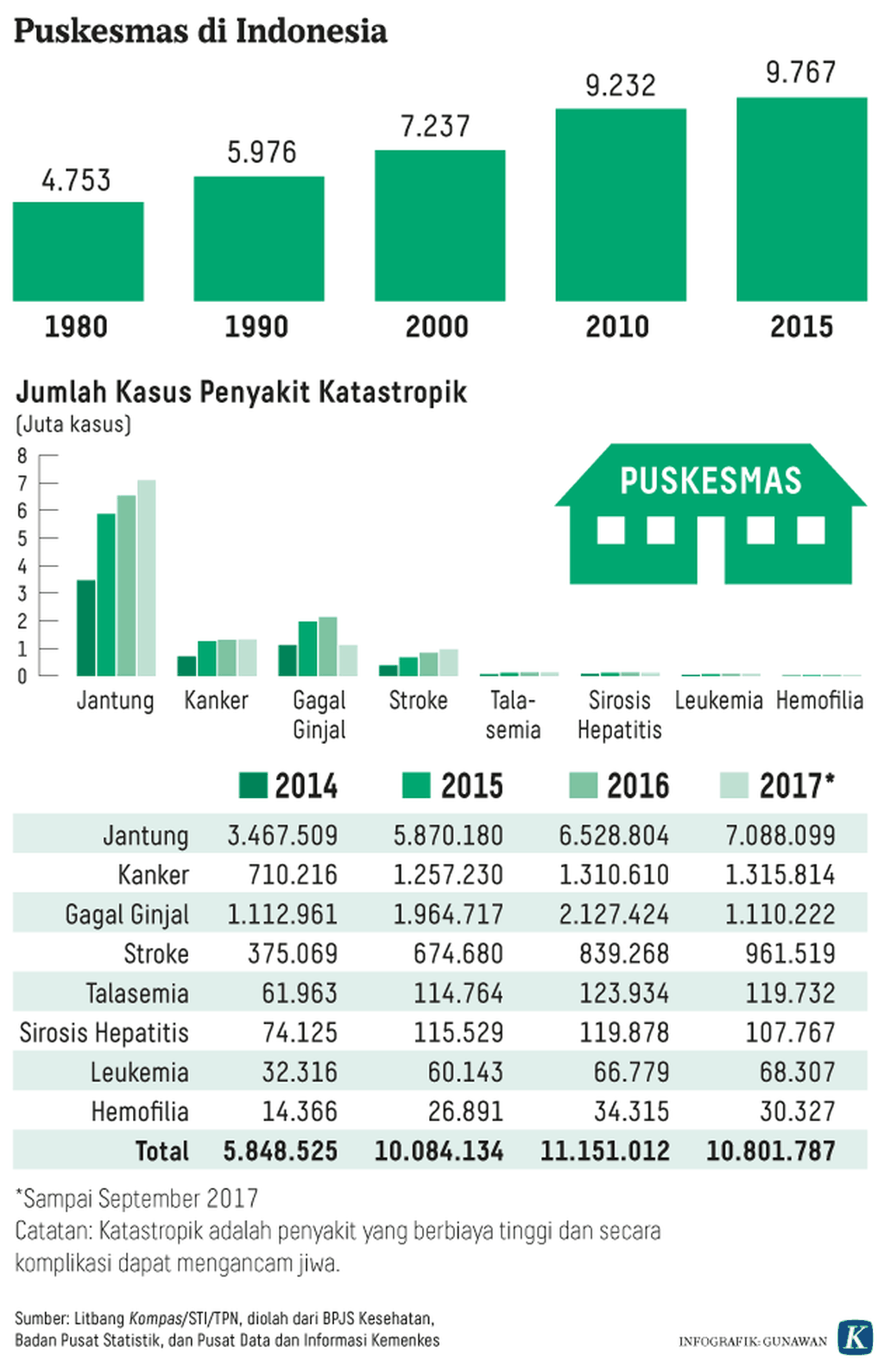
Puskesmas, or community health centers, are relied on as the spearhead of community health service. Based on the Indonesian Health Profile 2016 issued by the Health Ministry in 2017, there are 9,767 Puskesmas throughout Indonesia, and there are 16,527 doctors, 6,618 dentists, 120,081 midwives and 98,864 nurses and health workers placed in Puskesmas.
However, a number of extraordinary occurrence (KLB) diseases have still spread. Aside from remote areas, KLBs have also occurred near centers of administration. The number of patients seeking treatment in Puskesmas and hospitals continues to increase year after year.
The birth of Puskesmas dates back to the Dutch colonial era, according to factsanddetails.com. The aim, at the time, was to maintain the health of plantation workers. In its development, community health efforts started with smallpox and cholera vaccinations.
The Puskesmas concept was born in 1968 in a national health work meeting in Jakarta. At the time, certain activities, like mother and child health centers and medication centers, as well as infectious disease prevention and eradication, among others, were being run separately from each another. Thus, the idea of integrating all first-level services was born.
Puskesmas were first opened in 1969 when Pelita I was founded. The challenge was to tackle various health problems plaguing society at the time, such as the high number of smallpox, malaria and tuberculosis cases, as well as the low nutritional status among infants and pregnant women, which contributed to high infant and maternal mortality rates. According to records, 120 to 150 out of every 1,000 babies died before reaching 1 year old.
In 1974, as stated in the book Mencatat Sejarah Kesehatan Nasional Indonesia Era 1973-2009 (Recording Indonesia’s National Health History in the 1973-2009 Era), in the time of Health Minister Prof. dr. GA Siwabessy, the World Health Organization (WHO) stated that Indonesia was smallpox-free. Puskesmas received its recognition in 1978 when the Alma Ata Declaration was planned. The main content of the declaration stated that basic health service would be the main strategy to achieve health for all as a manifestation of human rights. The government built Puskesmas in every corner of the country. At the end of Pelita II in 1979, there were 3,400 Puskesmas in Indonesia. In 1999, the recorded infant mortality rate was down to 46 per 1,000 births and the maternal mortality rate was 373 per 100,000. At that time, Posyandus (integrated health posts) also started shutting down.
Since the Reformation Era, the work partner of Puskesmas, the Family Welfare Movement (PKK), received a lot of criticism, despite the state-mobilized women’s organization being the backbone of the management of Pasyandu. The economic crisis in Indonesia caused volunteerism to decline, meaning that the role of the community also faded.
The era of regional autonomy affected the performance of Puskesmas. Because of a claimed lack of funds, many regional administrations did not allocate operational costs — in fact, they made Puskesmas a source of locally generated revenue. As a result, Puskesmas became only a polyclinic, and community health programs were not implemented. It is no wonder that KLB infectious diseases have been spreading.
The terrain and high transportation costs in Papua, Maluku or in the suburbs of Kalimantan, have made it difficult for people to access health care. Likewise, access to health care from people in remote regions has been hampered by the shortage of budget and the lack of interest from doctors.
The government’s commitment, particularly from regional administrations in the era of regional autonomy, is expected. The poor should not fall ill first before receiving the government\'s attention.