A century ago, influenza became a global pandemic and a serious health threat that took 50 million lives. Even today, the world is still often at a loss in the face of new pandemics.
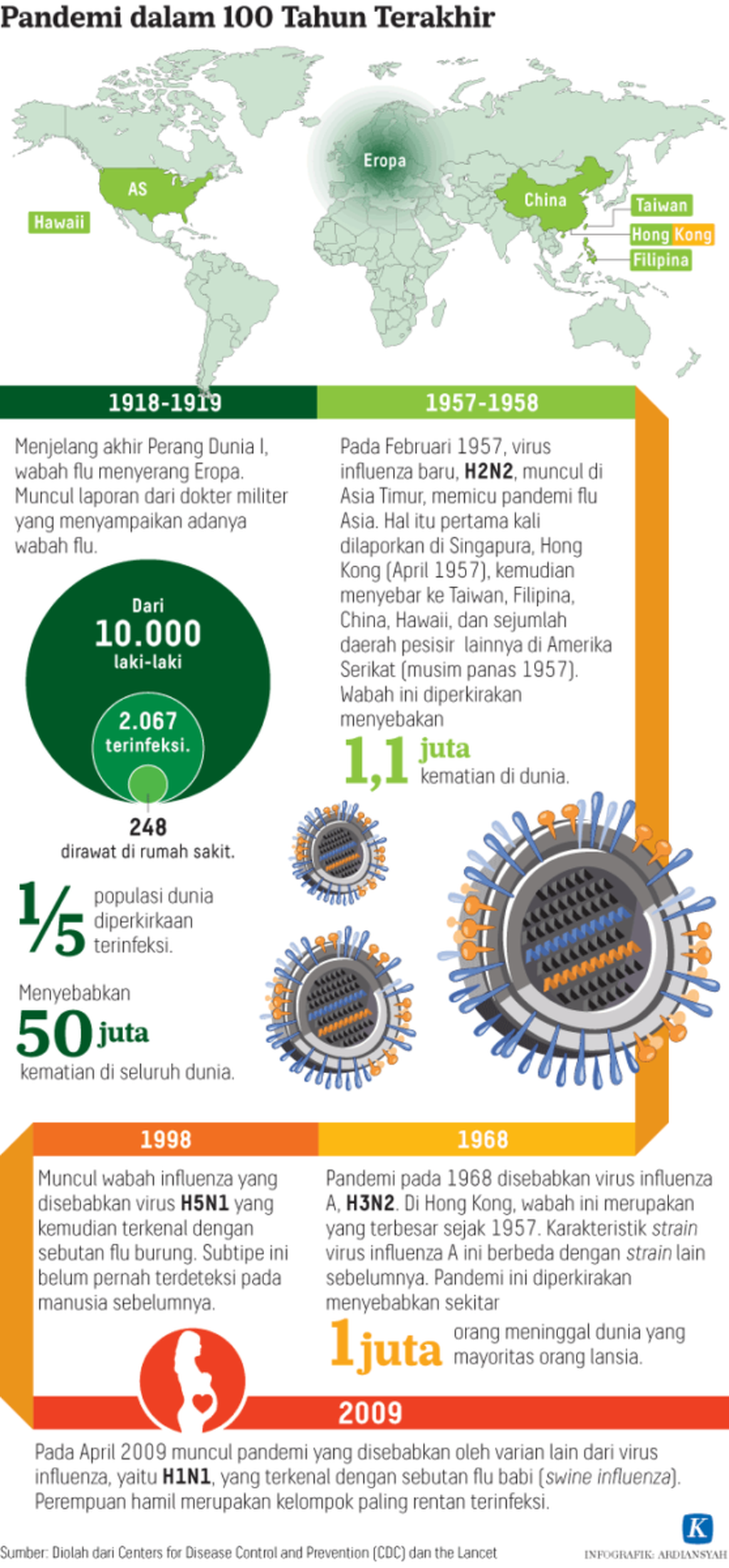
One hundred years ago, influenza became a global pandemic. At the time, it was estimated that a fifth of the global population was infected, and around 50 million people died. Today, new infectious diseases are lurking in every corner, waiting for the moment when we become careless, both with our individual immune system and with our preventive healthcare system.
The influenza pandemic one century ago occurred in three waves. In late 1917, a US military pathologist warned that a new, deadly disease was waiting to happen. The first official report of the disease came from Haskell County in Kansas in 1918. The first epidemic is thought to have broken out at Funston Camp, Fort Riley, Kansas, where US troops were trained for deployment in World War I. Before midday on March 4, 1918, 100 military personnel were hospitalized.
The second wave occurred when sick US soldiers were deployed to battlefields in WWI and triggered the death of millions in October and November of the same year. The disease was triggered by a deadlier virus. The third wave of a less severe disease took place in 1919.
Science of the era could not comprehend the disease. Scientists needed 15 more years before they could scientifically prove that the influenza pandemic had been a viral infection. The influenza virus was alien to the human body, which did not yet have the proper antibody against it. Many lives were lost. The spread of the disease far outpaced the measures taken to curb it and to treat the infected.
There have been several more influenza pandemics since, including the 1957 pandemic in Singapore, Taiwan, the Philippines, China, Hawaii and Hong Kong (1957 and 1968). Around 30 years later, in 1998, H5N1, or bird flu, spread to many countries. In 2009, there was H1N1, or swine flu. In the US, pregnant mothers were highly prone to H1N1 infections.
The influenza pandemics over the past 100 years have been well documented in the scientific journal The Lancet.
As bouts of influenza stroke in the past century, preventive and curative efforts have been developed through research. New medicines and vaccines have cropped up.
Indonesia One Health University Network coordinator Wiku Adisasmito said proper skills to prevent, detect and respond to diseases were important in the face of pandemics. With regard to influenza, countries are quite skilled at detecting pandemics but struggle to prevent them. For instance, thermal scanners at airports are only used during outbreaks. When there is no outbreak, the scanners are not put to use. The authorities are letting down their guard – despite the high speed at which people move around the world in great numbers these days.
A person can travel between continents in less than 24 hours and have contact with many people along the way. With poor preventive capacity, the risk of a plague is huge.
However, influenza is different from emerging infectious diseases, a majority of which come from animals (zoonotic). In the influenza pandemics of the old time, we only faced one type of disease at a time. The challenges posed by emerging infectious diseases are different. We now face many types of previously unknown diseases. Among them are HIV/AIDS, severe acute respiratory syndrome (SARS), the Middle East respiratory syndrome coronavirus (MERS-CoV) and Zika.
After disappearing for a long while, infectious diseases can reemerge and spread again. One example is Ebola, which first emerged in Africa in 1976 and then again in 2014, when it became widespread and took many lives. The Ebola pandemic tore down the economy in African countries where it spread.
Detection ability
Countries across the world lack in their capacity to detect emerging infectious diseases, not least because of poor collaboration among authorities concerned with public health, animal health and forestry. Detection and prevention abilities in each sector are poor; the “detection capability is good in only a few countries,” Wiku said.
Uncertainty in the face of emerging infectious diseases is caused by low awareness among government leaders, medical human resources and the public. The limited approach to tackling health problems is the result of healthcare education that does not prioritize a comprehensive approach in tackling diseases. When these healthcare professionals enter government administration, they fail to collaborate effectively across agencies.
Now, countries around the world understand that emerging infectious diseases must be tackled with a “one health” approach that combines public health and animal health. If the government pays huge attention to promotive and preventive healthcare, the National Five-Year Development Plan (RPJMN) should ideally include a commitment to tackling disease risk factors.
An initiative from global health organization Vital Strategies, titled “Resolve to Save Lives”, maps the preparedness of countries to face emerging infectious diseases. Data used in the mapping include the assessment result of the implementation of international healthcare regulation (IHR) 2005 by the Joint External Evaluation (JEE) team developed by the World Health Organization (WHO).
The mapping shows that Indonesia’s score for emerging infectious disease preparedness is 64, on a scale of 0 to 100. Thus, Indonesia’s prevention, detection and response capabilities must be improved – especially in the aspect of prevention. The derivative components of the prevention aspect should also be improved, including regulation, funding, coordination, communication, IHR advocacy, anti-microbe and zoonotic diseases’ resistance and food safety.
Action plan
“It is time for the global community and countries to improve their preparedness,” former US Center of Disease Control and Prevention (CDC) chair and current Resolve to Save Lives CEO and president Tom Frieden said in a written statement.
The JEE report on Indonesia’s core IHR capacity, compiled by the WHO in 2017, recommends that the Indonesian government devise a national action plan to implement IHR 2005 measures. The action plan must involve various ministries as well as national and regional agencies. The core capacity of various agencies in tackling emerging infectious diseases must be evaluated and improved.
Health Ministry Director General of Disease Prevention and Control Anung Sugihantono said Indonesia had implemented IHR 2005. IHR is a cycle of improvement in preparedness against public health emergencies. Contingency plans are in place at some of the country’s entry points in preparation for potential public health emergencies.
As a follow-up to the IHR implementation assessment by the WHO’s JEE team, presidential instructions on prevention, detection and response to pandemics and nuclear, biological and chemical emergencies are being prepared. Wiku said he hoped the presidential instructions would be a first step by the government to coordinate cooperation to tackle emerging infectious diseases.