Problems Related to Covid-19 Vaccines
As people, both nationally and globally, get bored with social restrictions, the positive results of vaccine trials are considered a breath of fresh air amid all the uncertainty
The first anniversary of the Covid-19 pandemic will be greeted with a Covid-19 vaccination program. As people, both nationally and globally, get bored with social restrictions, the positive results of vaccine trials are considered a breath of fresh air amid all the uncertainty.
The Indonesian government has also announced an estimation of 107 million people who will get the first priority of vaccines and it is projected to start in the third week of January 2021. Even, theatrically, as many as 1.2 million doses of the Sinovac vaccine arrived in Indonesia earlier this week to ensure its implementation.
Also read: Vaccines as Public Goods
However, with all its potential, vaccines are not the ultimate weapon to confront this pandemic. There are many limitations and potential problems that must be mitigated from the start of the preparation of its implementation plan. How priorities are formulated, distribution and data collection plans, logistical supplies, and social justice issues can become serious problems in the coming months if not properly anticipated.
Priority discussion
The first issue is the priority list of vaccine recipients. The main priority criteria are young age (19-59 years), do not have comorbid diseases, are not pregnant, and have never been infected with Covid-19. The three criteria are attached to groups of health workers, public area workers, educators, community leaders, and participants of the National Health Insurance (JKN) program, especially those who receive contribution assistance.
This priority list is different, if not considered the opposite, of priority lists compiled by other countries. The United Kingdom and the United States, for example, place people aged 50 years and over and those at high risk of developing severe symptoms and death if infected as their top priority after health workers.
Also read: Bio Farma Ready to Process Vaccine Raw Materials
The difference lies in the type of vaccine selected. Pfizer and Moderna registered more than 7,000 people over 65 years of age and more than 5,000 people under 65 with comorbidities. This was not done in the Sinovac trials, which only tested the vaccine on people aged 19-59 years, so it has not been able to provide valid evidence regarding its use in the elderly and people with comorbid diseases.

President Joko Widodo ensured that the Covid-19 vaccine was free for the Indonesian people. The statement was conveyed from the Merdeka Palace online, Wednesday (16/12/2020).
Then, does this vaccine provide any benefit if people who are at high risk do not get priority? The benefits still exist, but must be critically understood and anticipated. If not, the policy to be set will be wasteful. Not cost effective. Not resource effective.
The efficacy of vaccines reported in various studies is the efficacy of preventing mild-moderate symptoms, severe symptoms, and death. Moderna claims that its efficacy in preventing the appearance of symptoms related to Covid-19 has reached 94.1 percent. Even, if the outcome of the efficacy is changed to "efficacy in preventing severe symptoms," the efficacy jumps to 100 percent. Likewise, the Pfizer and BioNTech release claim 95 percent efficacy.
Also read: Vaccine Supply Follows WHO Standards
What should be noted is that there is no evidence of efficacy in infected people, but are asymptomatic. In fact, being infected with Covid-19 is often asymptomatic, but still has a high potential of transmitting to others. People who are young and do not have comorbid diseases tend not to show symptoms of infection -- commonly referred to as people without symptoms. However, they have the potential to become a source of transmission to others.
If only this group is vaccinated, while the high-risk groups do not receive priority, the potential for disease transmission remains high. Precisely those who are at high risk have the potential to need hospital services and will continue to burden health services. If the burden of health services is not reduced optimally, the economic burden will remain stagnant, even increase. Or at least, it will be a policy that is not cost effective.
High risk protection
If this priority remains to be implemented, additional policies will be needed by identifying high risk groups appropriately. Whoever belongs to this group must be formulated in a joint consensus. How big the proportions are, and where they are spread, must be able to be mapped.
Also read: Vaccination Pending Scientific Study
Second, they must be protected against potential of transmissions while promoting mobility restrictions, not mingling in crowds, and maintaining strict distancing. When the community is psychologically saturated, this is not a simple problem, let alone if there are economic needs that must be met. Therefore, after being mapped, this group must receive sufficient socioeconomic protection.
By doing so, the vaccination program with priorities like this does not just talk about the budget for fulfilling vaccines, but also the socioeconomic protection needs of people who are "disadvantaged" because they do not get the vaccine priority. If not, social injustice will arise and has the potential to raise new health problems in the community. And, with the disclosure of the Covid-19 social assistance corruption case, this step is very crucial to be prepared since the early stage.
Also read: Make Equal Access to Vaccines Happen
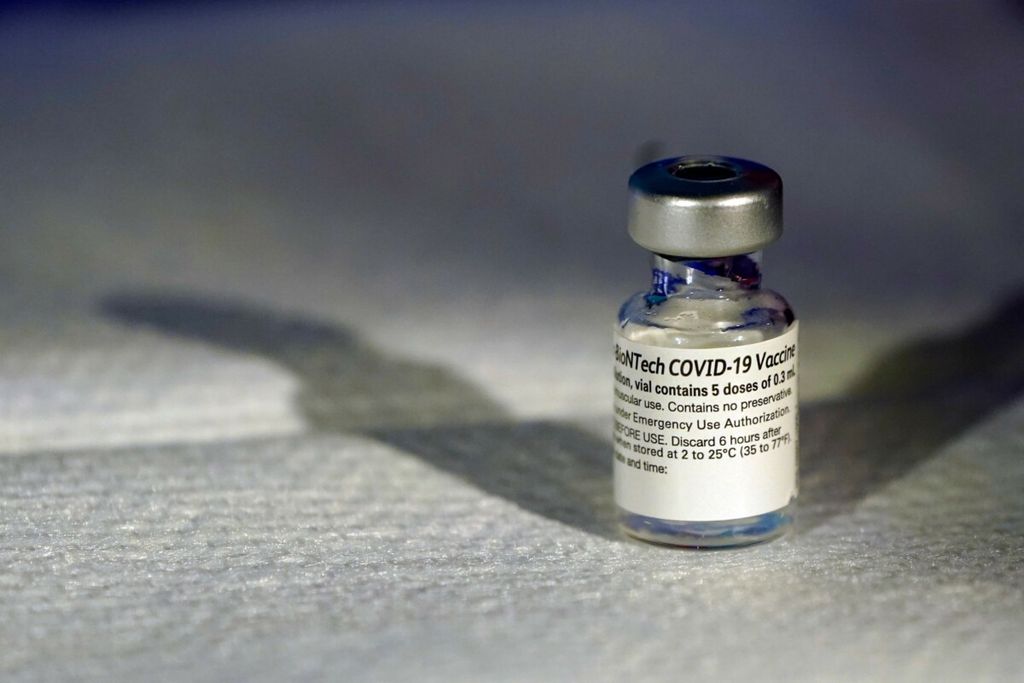
A vial of Pfizer COVID-19 vaccine that receive emergency use authorization is seen at George Washington University Hospital, December 14, 2020, in Washington, DC. - The United States kicked off a mass vaccination drive Monday hoping to turn the tide on the world\'s biggest coronavirus outbreak, as the country\'s death toll neared a staggering 300,000.
Production vs needs
The third problem is the balance between production and needs. Assuming that the 107 million targets require two doses of vaccine, plus a 15 percent wastage rate, the total requirement is 246.5 million doses.
The Research and Technology Minister had claimed the ability to produce one billion doses of vaccine per year, but this assumption seems to be exaggerated. Bio Farma\'s current production capacity is claimed to be around 16 million-17 million per month, but that also depends on supplies from Sinovac and will not be maximally achieved in the initial period. To achieve the total dosage requirement, it takes 14.5 months. Supplies of 6.6 million doses of vaccine from China only shorten it to 14 months.
Also read: What Needs to be Considered From the New Vaccine
Cooperation with other vaccine producers can shorten the achievement, especially for the independent vaccine groups. However, how to pit these priorities against the need for vaccines for high-risk groups -- who should be able to use them as an alternative? Moreover, these alternatives also have the potential to create new gaps among groups of people due to technical constraints on storage, distribution, price range, and infrastructure readiness.
Fairness of distribution
With the limited availability of vaccines and the existence of "mandatory" and "independent" groupings, the potential for imbalance and unfair distribution must be reduced to the minimum possible. How to maintain a balance on the availability of the two groups so that there is no vacancy in the “obligatory” group because more supplies are available in the “independent” group: 32 million vs 75 million.
The problem of swab and PCR (polymerase chain reaction) tests has provided meaningful lessons about price control and equitable distribution, and the potential for misuse of funds for procurement and distribution with a large amount of rupiah requires very close supervision.
Also read: Acceptance, the Key to Vaccination
The last problem is data collection. There are nearly 27 million JKN participants who receive contribution assistance (PBI). How good is the data currently available? The experience of sending social assistance and the wrong target on the Jamkesmas (the National Health Guarantee), Askeskin (the health insurance for the poor), and JKN PBI participation is an early warning for how data should be properly managed down to the grassroots.
Long before the priority list was announced by the central government, local governments up to the RT (neighborhood unit)/RW (neighborhood community) level have taken the initiative to compile a list of residents who receive the Covid-19 vaccines. How can the government data synchronize with data collected independently by residents? What if there are residents who have not been registered as JKN PBI participants, but are deemed worthy of receiving priority vaccines?

Ahmad Fuady
The government needs to communicate all of these things in a clear and transparent way. There is no need for any information to be covered up, even fabricating the good news without a clear scientific basis. The government must be able to put it in a balanced manner. The main key to controlling this pandemic comes from the public trust. Where can that trust be built?
From the policy gesture being taken -- one that is consistent, scientifically based, and transparent.
Ahmad Fuady, Lecturer at the School of Medicine, University of Indonesia.